Upper Cross Syndrome: What It Is, Why It Happens, and How to Fix It
If you spend most of your day sitting at a desk, driving, or looking at a screen, there’s a reasonable chance your body has developed upper cross syndrome — even if you’ve never heard the term.
It’s the most common postural pattern in clinical practice. It drives neck pain, shoulder tension, headaches, and upper back stiffness that most people attribute to stress, aging, or simply “sitting too much.” Those observations aren’t wrong — but they don’t explain the mechanism. And without understanding the mechanism, the treatment doesn’t hold.
The Pattern — What Janda Observed
Czech neurologist Vladimir Janda described upper cross syndrome in the 1970s as part of his broader work on muscle imbalance patterns. His
View of Upper Cross Syndrome
observation was that the muscles around the neck and shoulder girdle don’t dysfunction randomly — they follow a predictable pattern based on how the nervous system responds to sustained posture and load.
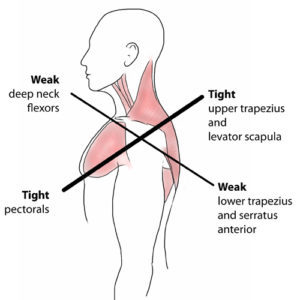
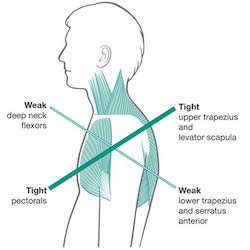
Some muscles tighten and overactivate. Others weaken and shut down. When these tendencies interact across the cervical spine and shoulder girdle, a cross-pattern of dysfunction emerges:
The tight and overactive muscles:
- Upper trapezius — elevates and compresses the shoulder girdle, contributes to neck compression
- Levator scapulae — pulls the cervical spine into extension and lateral flexion
- Pectorals (pectoralis major and minor) — pull the shoulders forward into protraction and internal rotation
- Suboccipital muscles — compress the base of the skull as the head shifts forward
The inhibited and underactive muscles:
- Deep cervical flexors (longus colli, longus capitis) — lose their ability to stabilize the cervical spine from the front
- Lower and middle trapezius — fail to retract and depress the scapulae, allowing them to wing and tip forward
- Serratus anterior — loses its role in holding the scapula against the rib cage
The result is a head that sits forward of the shoulders, a cervical spine under compressive load, shoulders that roll inward and forward, and a thoracic spine that rounds to compensate for all of it.
Why the Body Develops This Pattern
The human head weighs approximately 10–12 pounds in neutral position. For every inch it shifts forward of the shoulders, the effective load on the cervical spine increases significantly — some estimates put it at an additional 10 pounds of force per inch of forward translation.
Sustained forward head posture — from screens, desks, driving, or any activity that pulls attention forward — trains the nervous system to treat that position as normal. The muscles that hold the head forward shorten and tighten. The muscles responsible for pulling it back stop being recruited because the nervous system stops asking for them.
This is the same principle Janda identified across the body: the nervous system adapts to the position you spend the most time in. The adaptation that makes sense for short-term efficiency becomes a problem when it calcifies into a resting pattern.
The Postural Restoration Institute (PRI), founded by Ron Hruska in the 1990s, extended Janda’s work by asking a question Janda’s model didn’t fully answer: why does the pattern express differently from person to person — and why does it almost always express asymmetrically?
The answer lies in a fact of human anatomy that most clinicians overlook: we are not bilaterally symmetrical. Your liver is on the right side of your body. Your heart tilts left. Your diaphragm — the primary muscle of breathing — is larger and more dome-shaped on the right than on the left. These structural asymmetries mean the body has a built-in tendency to rotate, shift, and position itself in predictable ways. Most people, most of the time, have a dominant right side that is more extended, more externally rotated, and more pulled back — and a left side that compensates by doing the opposite.
In upper cross syndrome, this asymmetry shows up clearly. One shoulder sits higher than the other. The head tilts or rotates slightly toward one side at rest. The neck is tighter on one side than the other. The dominant shoulder — usually the right in right-handed people — is often more retracted and elevated, while the opposite side compensates with more protraction and forward rounding.
This isn’t random variation. It’s a predictable expression of the body’s underlying asymmetric organization playing out through the muscle imbalance pattern Janda described.
Why does this matter clinically? Because treating upper cross syndrome symmetrically — stretching both sides equally, strengthening both sides in the same sequence — often produces partial results. The dominant side of the pattern needs to be identified and addressed first. The inhibited muscles on the non-dominant side need to be activated in positions that account for where the body is actually starting from, not where it theoretically should be.
This is the contribution PRI makes to Janda’s framework: not replacing what he observed, but explaining the asymmetric driver behind it and providing a clinical system for addressing it in the correct sequence.
What Upper Cross Syndrome Actually Causes
The symptoms of upper cross syndrome extend well beyond the neck and shoulders. When the head is forward and the shoulder girdle is compromised, the downstream effects are predictable:
Neck pain and stiffness — the cervical spine is under chronic compressive load from above. The deep stabilizers that should be managing that load have been inhibited. The superficial muscles compensate by bracing — which means they’re always on, always working, and never fully recovering.
Cervicogenic headaches — headaches that originate from the cervical spine and suboccipital region rather than from vascular or hormonal causes. The compression at the base of the skull irritates the suboccipital nerve complex and refers pain into the head. These headaches are frequently misdiagnosed and treated with medication that doesn’t address the source.
Shoulder impingement — when the scapula tips forward and the shoulder rolls inward, the subacromial space narrows. Tendons that pass through that space get pinched with every arm elevation. Over time this contributes to rotator cuff tendinopathy and impingement syndromes.
Mid and upper back pain — the thoracic spine rounds to compensate for the forward head and protracted shoulders. The muscles along the thoracic spine are chronically loaded in a lengthened position, which produces the dull ache between the shoulder blades that most people associate with “tension.”
Jaw pain and TMJ dysfunction — the position of the head directly influences the position of the mandible. Forward head posture alters the resting position of the jaw and changes how the TMJ loads — contributing to clenching, grinding, and chronic jaw tension.
Breathing dysfunction — the pectorals and upper traps are accessory breathing muscles. When they’re chronically tight and overactive, they take over a greater share of the breathing load — which contributes to shallow, upper-chest breathing that keeps the nervous system in a low-level stress response.
Why Stretching Alone Doesn’t Fix It
The standard advice for upper cross syndrome is to stretch the tight muscles and strengthen the weak ones. That logic is directionally correct — but incomplete for the same reason it’s incomplete in lower cross syndrome.
Stretching the upper traps and pectorals without addressing why they’re overactivating doesn’t change the underlying pattern. They tighten again because the nervous system is still driving the same compensation. The deep cervical flexors and lower trapezius won’t consistently activate under strengthening exercises if the inhibitory signals keeping them offline haven’t been addressed first.
The sequence matters. Position first — restoring the cervical and thoracic mobility that allows the head to sit back and the scapulae to move correctly. Then motor control — retraining the deep stabilizers to activate in the right positions. Then progressive loading — building the strength and endurance that makes the correction hold under real-world demand.
Skip the first two steps and go straight to strengthening, and you’re loading a system that isn’t positioned to respond correctly.
How Upper Cross Syndrome Is Treated at Ashworth
The evaluation looks at the whole pattern — not just where it hurts. That means cervical and thoracic mobility, scapular positioning, breathing mechanics, and which side the pattern is expressing most strongly. The assessment identifies what’s driving the compensation before the treatment plan is built.
Chiropractic addresses the joint restrictions that both contribute to and result from the pattern — but the evaluation that precedes it is what makes the treatment work.
Dr. Matt Wilson has been training with the Postural Restoration Institute since 2020. His intake process includes a PRI-informed functional assessment that looks at breathing mechanics, stance position, rib cage orientation, and the asymmetric expression of the pattern before any treatment is planned. This is not a standard chiropractic evaluation. Most assessments identify where the restriction is. A PRI-based assessment asks why the body is holding that position — which produces a different answer and, in most cases, a different treatment sequence.
In upper cross syndrome specifically, this means identifying which side of the pattern is dominant before deciding where to start. Treating the cervical and thoracic restrictions symmetrically — without accounting for the asymmetric driver — is one of the reasons upper cross syndrome responds partially to standard chiropractic care and then reverts. The correction needs to address the pattern in the sequence the nervous system will actually accept.
Restricted thoracic extension is one of the most consistent joint findings in upper cross syndrome — when the mid-back can’t extend, the neck compensates by extending more than it should. Cervical restrictions compound the problem. Restoring mobility at both levels, in the correct sequence and starting on the correct side, changes the mechanical environment the muscles are working in.
One thing worth noting for patients who’ve been through standard upper cross syndrome treatment and plateaued: the treatment sequence that produces the best results often looks counterintuitive from a standard clinical perspective. That’s because the driver of the pattern is frequently in the lumbar spine and pelvis — not the neck and shoulders where the symptoms are. Addressing that driver changes the treatment entirely, and the results consistently exceed what the standard Janda-based approach produces.
For more on the Postural Restoration Institute framework and why asymmetry matters clinically, the PRI website and their course descriptions explain the clinical model in depth.
Physical therapy with Kelly Brown Gross, PT, WCS addresses the neuromuscular component — specifically retraining the deep cervical flexors, lower trapezius, and serratus anterior in the correct sequence and positions. These muscles don’t respond reliably to generic strengthening exercises because they’ve been inhibited long enough that the nervous system needs to be re-educated before loading makes sense.
Massage — particularly trigger point work in the upper traps, levator scapulae, suboccipitals, and pectorals — addresses the soft tissue component that resists both joint correction and neuromuscular retraining. Chronically overactive muscles develop trigger points that refer pain and maintain the guarding pattern. Releasing that tissue is often what allows the other work to take hold.
Most patients with upper cross syndrome have significant improvements in symptoms in 6–8 visits. Cases with longer chronicity, significant cervicogenic headache involvement, or secondary shoulder pathology may take somewhat longer. Ongoing home care exercises and awareness of the factors that cause upper cross and lower cross syndrome is necessary for full resolution.
Self-Assessment: Do You Have Upper Cross Syndrome?
A few observations that suggest this pattern may be present:
- Your head sits forward of your shoulders when you’re standing relaxed
- One or both shoulders roll forward and inward at rest
- You carry chronic tension in the upper traps and base of the skull
- You get headaches that start at the back of the neck and move forward
- Your upper back aches between the shoulder blades after sitting
- Stretching the neck and shoulders provides temporary relief that never lasts
- You’ve been told you have “tech neck” or forward head posture
None of these is diagnostic on its own. But the pattern is worth evaluating properly — because the longer it’s present, the more layers of compensation build around it, and the longer correction takes.
Frequently Asked Questions
Is upper cross syndrome the same as forward head posture? Forward head posture is one visible component of upper cross syndrome — the head position that results from the muscle imbalance pattern. Upper cross syndrome is the full pattern: tight upper traps, levator, and pectorals combined with inhibited deep cervical flexors and lower trapezius. You can have forward head posture without the complete upper cross pattern, but they’re closely related.
Can upper cross syndrome be permanently corrected? Yes — but it requires addressing the neuromuscular pattern, not just the symptoms. Patients who complete a proper correction sequence and maintain the movement habits it builds typically stay resolved. Passive treatment alone — adjustments, massage, stretching without retraining — produces relief that fades because the pattern reasserts.
How long does treatment take? Most patients see meaningful improvement within 4–6 visits and reach symptom resolution in 6–8. Neuromuscular re-education takes time however and home care exercises and awareness of the pattern and triggers is key to complete resolution. Cases with significant cervicogenic headache involvement or secondary shoulder pathology may take longer.
Is this related to lower cross syndrome? Often yes — and this is one of the most clinically important points about upper cross syndrome. Janda described upper and lower cross syndrome as frequently co-occurring because they’re driven by the same underlying nervous system tendencies. The pelvis tips forward in lower cross syndrome partly because the thoracic spine rounds to compensate — and the thoracic spine rounds partly because of what’s happening at the pelvis and hips.
From a PRI perspective, upper and lower cross syndrome are expressions of the same whole-body pattern playing out at different levels of the spine simultaneously. Treating the neck and shoulders without addressing what’s happening at the pelvis and hips is one of the most common reasons upper cross syndrome responds partially and then reverts. The body is one connected system — and the correction needs to account for the whole pattern, not just where the symptoms are.
Learn more about lower cross syndrome →
We’ll be publishing a dedicated article on why upper and cross syndrome need to be addressed together — and what that looks like in practice.
Do I need a referral? No. Iowa is a direct access state for both chiropractic and physical therapy.