Lower Cross Syndrome: What It Is, Why It Happens, and How to Fix It
Most low back pain isn’t a back problem. It’s a pattern problem — and lower cross syndrome is one of the most common patterns driving it.
The term was coined by Czech neurologist Vladimir Janda in the 1970s. Janda observed that muscle dysfunction doesn’t occur randomly — it follows predictable patterns based on how the nervous system is organized. Some muscles are prone to tightening and overactivation under load. Others are prone to inhibition and weakness. When these tendencies interact across the pelvis, a recognizable cross-pattern of dysfunction emerges: tight hip flexors and lumbar extensors running one direction, weak abdominals and glutes running the other.
That pattern — lower cross syndrome — is one of the most common musculoskeletal presentations in clinical practice. And it’s one of the most underdiagnosed, because the symptoms it produces (low back pain, hip pain, knee pain) are treated where they hurt rather than where they originate.
What Janda Got Right — and What We’ve Learned Since
Janda’s original model identified the pattern accurately. What it didn’t fully account for was the neurological driver behind it.
The Postural Restoration Institute (PRI), founded by Ron Hruska in the 1990s, extended Janda’s framework by incorporating a critical variable: the inherent asymmetry of the human body.
We are not bilaterally symmetrical. Your liver is on the right. Your heart tilts left. Your diaphragm moves differently on each side. These structural asymmetries mean we have a built-in tendency to weight-shift, rotate, and position our pelvis and spine in predictable patterns — and those patterns directly influence which muscles tighten, which weaken, and which compensation patterns develop over time.
PRI framing adds a layer beneath Janda’s observation: the asymmetric position the body defaults to determines which version of lower cross syndrome you’re expressing, which muscles are inhibited and why, and — critically — in what order they need to be addressed to actually correct the pattern rather than temporarily relieve it.
In practice, this means two patients with identical symptoms and identical diagnoses of lower cross syndrome may need completely different treatment sequences, because the positional driver underlying their pattern is different.
What’s Actually Happening in Lower Cross Syndrome
The pelvis sits at the intersection of the lumbar spine, hip joints, and sacrum. When the muscles controlling pelvic position become imbalanced — some pulling too hard, others not pulling enough — the pelvis tilts forward into anterior tilt and the lumbar spine increases its curve into excessive lordosis, the thoracic spine also compensates often leading to mid-back pain and neck pain.
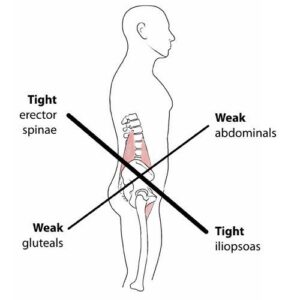
The tight and overactive muscles:
- Hip flexors (psoas, iliacus, rectus femoris) — pull the front of the pelvis down and forward
- Lumbar extensors (erector spinae, quadratus lumborum) — compress and extend the low back to compensate for the anterior tilt
The inhibited and underactive muscles:
- Glutes (gluteus maximus, medius) — fail to extend and stabilize the hip, allowing the pelvis to tip forward unchecked
- Deep abdominals (transversus abdominis, internal oblique) — lose their ability to create anterior pelvic stability
The result is a pelvis that is chronically tipped forward, a lumbar spine under constant compressive load, and hip joints that are being asked to function from a mechanically compromised position.
This is why lower cross syndrome doesn’t just cause low back pain. The downstream effects are predictable:
- Hip pain and bursitis — the hip joint is compressed and poorly positioned
- SI joint dysfunction — pelvic instability loads the sacroiliac joint asymmetrically
- Knee pain — altered hip mechanics change how load is transmitted to the knee
- Hamstring tightness — the hamstrings compensate for inhibited glutes and are chronically overloaded
- Foot and ankle problems — altered lower limb mechanics change how force is absorbed from the ground up
The patient presents with low back pain. The driver is a pelvic pattern. The symptoms are downstream consequences.
Why Treating the Symptoms Doesn’t Work
The most common treatment approach for lower cross syndrome is to stretch what’s tight and strengthen what’s weak. That logic is directionally correct — but incomplete.
Stretching hip flexors without addressing why they’re overactivating doesn’t change the underlying pattern. They tighten again because the nervous system is still driving the same compensation. Strengthening glutes in isolation without addressing the inhibitory signals keeping them underactive produces limited carry-over because the inhibition pattern reasserts under load.
The PRI contribution to this problem is identifying that the inhibition of the glutes and deep abdominals in lower cross syndrome is often driven by a positional pattern — specifically the body’s tendency to extend and externally rotate on the right side while collapsing into the left — that needs to be addressed through specific positioning and breathing strategies before the strengthening work can take hold.
In plain terms: you can’t strengthen a muscle your nervous system has decided to turn off. You have to change the position first.
How Lower Cross Syndrome Is Treated at Ashworth Clinic
The first step is an evaluation that looks beyond the symptom. Dr. Wilson’s intake process includes a PRI-informed functional assessment — evaluating breathing mechanics, stance position, pelvic orientation, and movement patterns to determine which version of the pattern is present and what is driving it.
This is not a standard chiropractic intake. Most evaluations identify where the restriction is. This one asks why the body is holding that position — which produces a different answer and a different treatment plan.
Chiropractic addresses the joint restrictions that are both contributing to and resulting from the pattern — lumbar, thoracic, and hip joint mobility that is limited by years of compensation. Restoring that mobility changes the movement environment the muscles are working in.
Physical therapy with Kelly Brown Gross, PT, WCS builds the neuromuscular re-education that makes the correction hold. The work follows the correct sequence: positional reset first, then breathing and motor control, then progressive loading of the glutes and deep abdominals in positions where the nervous system will actually let them activate.
Kelly sees one patient at a time, one hour at a time. That ratio matters for lower cross syndrome because the assessment needs to identify exactly which muscles are inhibited, which are compensating, and in what sequence the correction needs to happen. That level of precision doesn’t fit a 20-minute PT slot with three patients in the gym simultaneously.
Most patients with lower cross syndrome have substantial symptom reduction in 6–10 visits. Not months of ongoing care — a defined plan with measurable progress benchmarks and a clear endpoint. Let’s not overlook the connection to another one of Janda’s patterns: upper cross syndrome and the inevitable connection that is often incorrectly addressed separately. Upper and lower cross syndromes do not exist in isolation and must be addressed as such.
Self-Assessment: Do You Have Lower Cross Syndrome?
A few observations that suggest this pattern may be present:
- Your lower back feels stiff or compressed, especially after sitting or first thing in the morning
- Your hip flexors feel chronically tight despite regular stretching
- You have difficulty fully activating your glutes during exercise
- You’ve been told you have an anterior pelvic tilt or excessive lordosis
- Your low back pain is relieved temporarily by stretching but always returns
- You have recurring hip, SI joint, or knee problems without a clear structural cause
None of these is diagnostic on its own. But if several apply, the pattern is worth evaluating properly — because treating the symptoms without addressing the pattern is why low back pain becomes a chronic condition for so many people.
Frequently Asked Questions
What causes lower cross syndrome? Prolonged sitting is the most common driver — hip flexors adaptively shorten in the seated position while glutes are mechanically unloaded. Over time the nervous system recalibrates around that position. Poor movement patterns, asymmetric loading from sport or work, and the body’s inherent postural tendencies all contribute.
Can lower cross syndrome be fixed permanently? Yes — but it requires addressing the neuromuscular pattern, not just the symptoms. Patients who complete a proper correction sequence and maintain the movement habits it builds typically stay resolved. Those who only stretch and foam roll tend to cycle back.
How long does treatment take? Most patients see meaningful change in 4–6 visits and reach symptom resolution in 6–10. Cases with longer chronicity or significant secondary dysfunction may take somewhat longer.
Is lower cross syndrome the same as anterior pelvic tilt? Anterior pelvic tilt is one of the visible signs of lower cross syndrome — the pelvic position that results from the muscle imbalance pattern. They’re related but not identical. You can have anterior pelvic tilt without the full lower cross pattern, and lower cross syndrome involves more than just pelvic position.
Do I need a referral to be seen? No. Iowa is a direct access state for both chiropractic and physical therapy. You can schedule directly without a physician referral.
Schedule an evaluation or call 515-225-4002.

Your Path to Wellness Begins Here!
Our experts in chiropractic, physical therapy, acupuncture, and massage therapy work as a team to provide holistic care that meets your specific needs. Book your appointment today and experience coordinated care.
Dr. Matt and the entire staff have been GREAT! I went in for some issues I was having with my neck and back and Dr. Matt also helped me with some other issues I was having with my calf and shoulders that have made a HUGE improvement in my overall health and comfort.I highly recommend using Dr. Matt!
Dr. Matt has done wonders for me and I recommend him highly – I can’t say enough good things about him. Dr. Matt and staff are good people and will take great care of you.
I really love it here! They are very friendly and I feel Dr. Wilson is giving me great treatment! I also don’t feel pressured into coming back too frequently. The adjustments are great! Great office!
Dr. Matthew squeezed me in on short notice and took very good care of me. He was very thorough and didn’t just adjust me and let me walk out. Amazing experience here and the receptionist is a sweetheart.
Very professional and in depth consultation. These people seem to genuinely care about people’s health and progress.
My family have used chiropractic and physical therapy services here and every one of us have had excellent outcomes. I wouldn’t go anywhere else these folks are as good as it gets.